

Vitamin C plays an essential role in the formation of collagen. A deficiency in vitamin C can lead to scurvy, manifested by blood vessel fragility, fatigue, and, rarely, death. Today, scurvy is rare in developed countries. Therefore, to diagnose scurvy requires a high index of suspicion. This will be illustrated by our patient of interest.
A 66-year-old man presented to the emergency department (ED) with worsening bilateral leg swelling and bruising throughout his body. His past medical history was notable for a bowel resection with colostomy secondary to colorectal cancer, currently in remission. The bruising and swelling began two weeks prior without any inciting events. He denied taking blood thinners or non-steroidal-anti-inflammatory-drugs. He had no personal or family history of bleeding disorders. None of his previous surgeries were complicated by bleeding issues. Extremities showed large ecchymoses over left thigh and bilateral ankles, and hematoma over right patella. There were no perifollicular hemorrhages seen on skin examination. His hemoglobin was 13.5 g/dL and his platelet count was 145x109/L. A computed tomography angiography of his lower extremities revealed intramuscular hematomas in the calves, left adductor compartment and left sartorius. A venous ultrasound of bilateral lower extremities was unremarkable. He was advised to follow up with a hematologist outpatient.
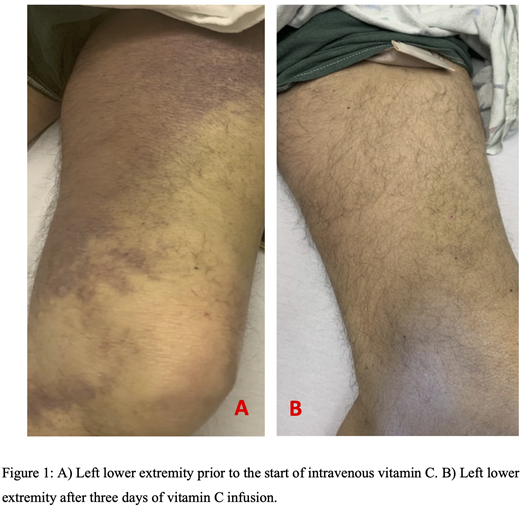
Ten days later, the patient reported worsening swelling and pain of his lower extremities and was advised to visit the ED (FIGURE 1A). His Hgb dropped to 10.8 g/dL. An extensive factor workup showed: factor VIII activity of 421.7% (ref range: 55-200), factor IX activity of 104% (ref range: 70-130), factor XI activity of 68% (ref range: 55-150), and von Willebrand factor activity of 355% (ref range: 55-200). Factor V, X and XIII were within normal limits. Other possible etiologies including vitamin K, HIV, hepatitis panel, antinuclear antibody and extractable nuclear antigen antibodies panel were normal. His activated partial thromboplastin time (aPTT) was prolonged at 44 seconds (ref range 25-37). The dilute Russel's viper venom time (dRVVT) was abnormal and his dRVVT/dRVVT-phospholipid ratio was greater than 1.3 or greater, indicative of a lupus anticoagulant. Beta-2 glycoprotein 1 antibodies and anticardiolipin antibodies were normal. Bleeding due to prothrombin (factor II) deficiency in the context of lupus anticoagulant has been reported (2). However, his factor II level was normal. Meanwhile, his Hgb fell to 6.9 g/dL, indicative of ongoing intramuscular bleeding.
Upon further investigation by the consulting hematology team and registered dietitian, there was a concern for severe malnutrition, evident by substantial loss of subcutaneous fat and muscle mass. The patient revealed that he consumed six twelve-ounce cans of beers nightly. His diet was minimal in fruits and vegetables. One month prior to his admission, he had worsening fatigue, brittle nails and gum bleeding. His folate level was 2.0 ng/mL (ref range >3.9) and his albumin level dropped to 2.1 g/dL (ref range 3.5-5). His vitamin C level resulted < 0.1 mg/dL (ref range 0.4-2). He was started on three days of intravenous vitamin C, one gram per day. His hematoma and bruises dramatically improved (FIGURE 1B). As a result, a diagnosis of scurvy was made. On discharge, he was transitioned to oral vitamin C and advised to follow up with his hematologist outpatient.
Scurvy is often viewed as a disease of the past. Yet, according to a national survey between 2003 and 2004, the prevalence of age-adjusted vitamin C deficiency is 7%. At risk patients include the elderly, institutionalized populations, alcoholics, and severe psychiatric illness leading to poor nutritional intake. Therefore, a dietary history of the patient should be obtained. Vitamin C contributes to the structure of blood vessels through its involvement in collagen synthesis. Characteristic signs and symptoms of scurvy feature fatigue, oral findings (spontaneous bleeding, gum retraction) and cutaneous abnormalities (petechiae and lesions). Rarely, it can lead to spontaneous intramuscular hematoma. The prognosis of scurvy is excellent, and the response to vitamin C is dramatic.
This case illustrates the need to consider scurvy in diagnosing bleeding cases. A high index of suspicion remains integral in diagnosing scurvy to avoid expensive and lengthy workup.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal